
Project Data
Zimmer Gunsul Frasca Architects, LLP (ZGF)
Architects
Oregon Health & Science University, Portland Oregon, USA (OHSU)
Client
39,292 m2 (401,412 sq. ft.)
Building area
Structural system (steel) grid varies due to existing below grade parking structure. Maximum bay size is 42’-9” x 28’-0” (13.03m x 8.53m) and smallest (at corners) is 20’-5” x 16’-6” (6.22m x 5.03m). To improve grid spacing, there are some transfers of columns to the parking levels via angled columns. Lateral seismic system is a moment frame. Two stair cores are off center and grouped with elevators (split between public and patient/staff), main mechanical/heating ventilation air condition, HVAC, shafts, stacked electrical and technology rooms. Smaller plumbing risers are adjacent to structural columns.
Floor to floor heights: Generally, 15’-0”/4.57m, increased at podium levels (16’/4.88m), first floor (20’-10”/6.35m) and the interstitial mechanical level (24’/7.32m)
Location of primary mechanical and electrical systems, those typically found in a Central Plant, are described later under “System Organization.”
Primary System
Non-loadbearing interior walls and mechanical electrical plumbing, MEP, distribution
Secondary System
Medical equipment (movable and fixed), office equipment, computer technology, furnishings and art.
Tertiary System
Sustainability
The project was certified as LEED Gold® by the U.S. Green Building Council.
Start of design 2014
Groundbreaking 2016
Opening 2019
Project Schedule
Introduction & Background
Oregon Health & Science University is a nationally prominent research university and Oregon’s only public academic health center. It educates health professionals and scientists and provides leading-edge patient care, community service and biomedical research. In 1919, the University of Oregon Medical School (OHSU's predecessor) moved from downtown Portland to its present location on Marquam Hill in Southwest Portland. In 2003 OHSU begin developing a campus along the Willamette River connected to Marquam Hill with the Portland Aerial Tram. In 2006 OHSU opened its first new building on the South Waterfront campus, the Center for Health & Healing (CHH) including new ambulatory services, faculty clinics and underground parking below the building and a vacant block to the south. Since then, riverfront development has continued with new research, education (dental school), and outpatient facilities.
The site for this case study, Center for Health & Healing South, (now called CHH-2) was on top of a 3-level underground parking structure and across the street from the original CHH (now called CHH-1). The building’s massing was set by City of Portland zoning regulations as follows: Level 1-4 are a full city block (200’ x 200’/ 61 m x 61 m) and upper floors are 200’/ 61m in east-west direction and 115’/ 35 m in north-south direction.
The building program was varied and included:
Clinics
Digestive health
Pre-operative
Clinical laboratory & Outpatient Blood Draw
Pharmacy
Outpatient
Compounding
Shelled space (6% of floor area including entire 6th floor space of 5th floor)
Surgery and interventional procedures suites
Extended stay outpatient rooms
Women’s health
Multi-digestive health
Knight Cancer Institute
Clinics & Diagnostic Imaging
Infusion
Cancer trial clinics (research)
Research offices
Support services including sterile processing, food service, staff facilities, and central plant/primary mechanical and electrical services for the three-building complex.
A primary design challenge was to accommodate these various programs (and potential future programs) in a multi-story building with the uniformly positioned vertical elements, (structure, circulation, and mechanical risers).
The Center for Health & Healing 2 demonstrates the Open Building approach in a healthcare building, although the term “open building” was not used in the design process. A primary project goal was long-term ability of the building to accommodate both changes in the initial program’s needs and to allow for future new programs.
The design process
Client goals were clearly stated at the outset:
Incorporate future trends in design with capacity to accommodate varied and changing uses.
Drive value from each functional and operational component.
Maximize the use of products and labor from the state of Oregon to the extent possible.
Embrace and push Lean design and construction principles.
Reap maximum value of a fully integrated team that inspires creativity, collaboration, and innovation reflective of the ambitious nature of the clients’ facilities.
OHSU also was looking for a design team and individuals who are willing to bring innovation to project delivery.
OHSU desired an integrated team with a proven track record of working together. Therefore, architects, contractors and consulting engineers self-selected to form teams prior to proposal submission. The selected team consisted of Zimmer Gunsul Frasca Architects LLP, Hoffman Construction, Affiliated Engineers Inc. (mechanical and electrical) and KPFF Consulting Engineers (structural and civil) plus specialty consultants. The major team members had successfully worked together on several projects, including for OHSU.
As an extension of the “integrated team,” a design process was developed that had two unique aspects:
An Integrated Project Delivery approach was developed by OHSU, ZGF and Hoffman. This involved the co-location of the owner, architect, engineers, general contractor and major sub-contractor team members in a Co-Location Space of over 100 workstations, from early design through construction, in temporary facilities adjacent to the construction site. This facilitated rapid and deep analysis of design issues by all parties including capacity to accommodate varied and changing uses. The colocation fostered communication among the owner, design consultants, general contractor and trade partners who were brought onto the project in the design phase.
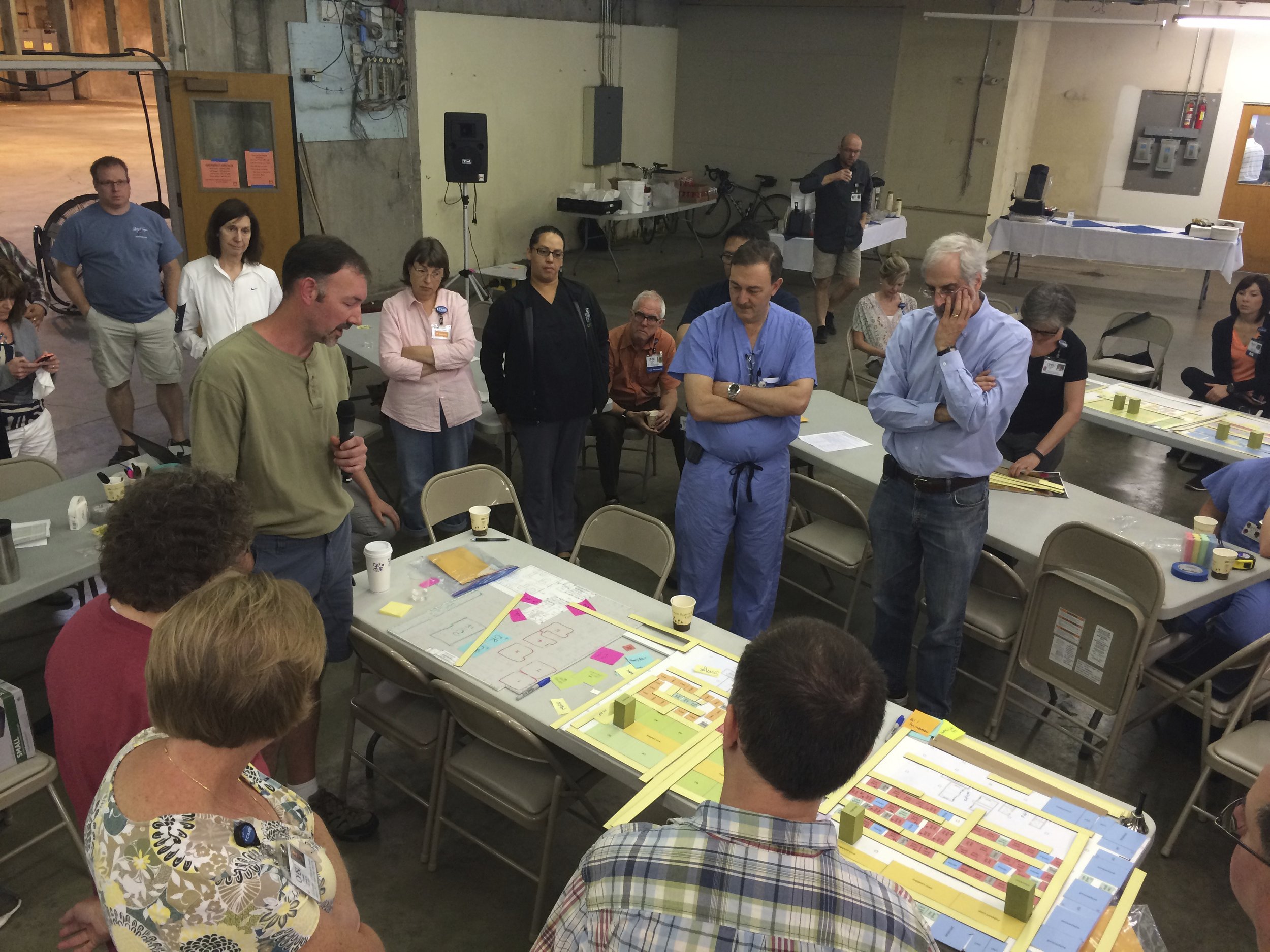
Nine rounds of Integrated Design Events (IDE’s) were orchestrated to develop Lean Process Improvements (LPI) of medical operations and building design. Nine IDE’s involving hundreds of stakeholders resulted in clearly defined goals, operational improvements and a better understanding of budget, costs, and schedule. Early events defined current state of operations and then developed future state operations. In later events, participants walked through full-scale mockups of entire clinical departments in a 30,000 sf (2,800 SM) warehouse to get a feel for “a day in the life” and fine tune details in individual rooms. A description of an IDE in early schematic design is described below under “Space Planning Process/IDE Events.”
The result was a design that not only accommodated opening day clinical processes but is adaptable to both incremental medical process improvements and major renovations. Another design goal was emphasis on a healing environment, patient experience and taking advantage of the excellent views. This helped drive floorplans that were more open and understandable, which in turn meant more adaptable to change.


Development of open building concepts
As noted previously, the term “Open Building” was not used. However, project goals and design processes had many parallels to “the Open Building approach,” including capacity analysis and separation of Base Building and Infill.
Concept Planning:
The project team evaluated buildings with similar programs for lessons learned starting with the existing and adjacent Center for Health & Healing 1. CHH-1 had identical floorplates, similar programs and had experienced some renovations since it’s design in the early 2000’s. Strategies to accommodate varied and changing uses were developed within constraints (e.g., zoning code envelope, existing parking structure below, and connection points via a pedestrian bridge and service tunnels to other OHSU buildings). A primary strategy was the grouping of building system risers, (HVAC, system piping, plumbing, electrical and technology), with fixed vertical circulation cores, (stairs, public and private elevators). These fixed elements are located off-center on the building floor plate to maximize an open loft-like floor area in the center of the building, offering capacity to accommodate varied and changing uses. Other strategies considered window mullion spacing, (~ 5 feet (1.5 m)), with alternating glazed and spandrel glass to accommodate a variety of room widths, all with daylighting and test fitting of a variety of planning modules for initial and potential programs.
Space Planning Process/IDE Events
The IDE events for each major program lasted up to three days and occurred from programming through design development phases. The key period for space planning coordination with the Base Building was in schematic design; therefore, a simple overview of an IDE in that period is provided. (Figures 3, 4 and 5)
IDE events were client-focused for OHSU staff, not the design team, to develop multiple layouts for each program within the proposed Base Building floorplate. OHSU participants included physicians, nurses, support and supply staff, and patient representatives. The design team was there to assist with problems and assure practicality including code compliance. These events, building on the “future state” of operations developed in programming, were tightly scheduled with goals and outcomes for each session (2-4 per day) with report-outs and discussion at the end of each session.
For clinical groups, participants included all specialties so that a standard clinic layout could be developed to allow clinics to be shared. OHSU also wanted new clinic layouts that also could be placed into the existing CHH-1 building. Similarly, the two procedure floors, surgical and interventional, worked together to develop similar concepts on their respective floors.
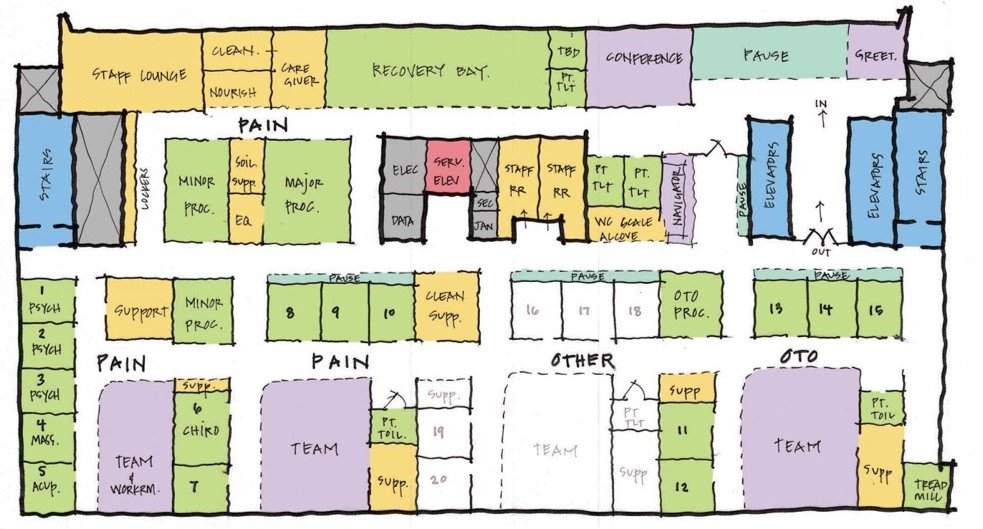
A typical IDE began with an overview of current project status and goals for the week. In early schematic design, each room in the space program was cut-out in colored coded illustration board at 1/8”=1’-0”(~1:100) scale. Five-room program sets were provided for development of multiple layouts on the given Base Building plan by different teams for tabletop or “gameboard” exercises. Options were compared to stated goals and data points, e.g., travel distances for patients and staff.
Between IDE days (and events), the design team developed plans of the gameboard options for further development. The design team also studied if modifications to the Base Building could or should be made that would improve layout and would coordinate those modifications between floors. At this point in the design process, these Base Building modifications might include adjusting the shape of a vertical mechanical shaft or changing access to an electrical room or stair to accommodate better clinical layouts.
When the number of options was reduced to two or three, full-size models of the clinical floors were built out of cardboard so that staff could walk through their daily operations and compare the options.
This is a very simplified description of the IDE process but illustrates how multiple layouts and programs were developed and tested for fit within the proposed Base Building (which could be slightly modified), demonstrating its capacity to accommodate varied and changing uses.








MEP system organization
Regarding MEP system organization, the project team worked together to evaluate dozens of system concepts with the goal of determining and implementing approaches that represented the best value to OHSU. Key considerations in these evaluations included:
Design systems that minimize operating costs and represented responsible use of energy and other resources.
Maximizing flexibility in the systems to accommodate a variety of program elements in the building and minimize the impact of future building modifications.
Locate major equipment in areas that allowed for appropriate service access and minimized disruption to surrounding programs.
Provide vertical distribution through the building that minimizes number of large vertical MEP risers on the floorplates yet provides appropriate access to systems.
Provide horizontal distribution on the floorplates that allows access to above ceiling equipment and systems that require regular maintenance and allows for future system modifications both without undue disruption to surrounding areas.
The team Co-Location space and early involvement of major subcontractors was an important element in facilitating real time and continuous intertrade concept development and coordination allowing for the optimization of both design and construction and the MEP systems. The existing parking structure below and ground floor program requirements coupled with a lack of adjacent land to satisfy MEP requirements necessitated central air conditioning plant functions be located higher in the building. The central plant also serves existing CHH-1 and the new Gary and Christine Rood Family Pavilion. Boilers, chillers and air handling units are located on an interstitial level at Floor 5 to directly serve downward to surgery and procedure suites (major air users), as well as the other adjacent buildings via below-grade connections and upward to other floors. Emergency generators and cooling towers are located at the roof level. Besides the grouping of large risers noted above, smaller risers for plumbing were placed adjacent to structural columns to maximize floor plan flexibility compared to risers in the middle of structural bays. Because CHH-2 provided central plant services to two other campus buildings, the vertical piping risers were larger than typical for a building of this size. Horizontal system runs were above suspended ceilings to serve respective floors mechanical, electrical and technology needs. Exceptions were plumbing drains that served the floor above and occasional electrical/technology runs accessing floor outlets in the floor above. Raised floors were not seriously considered due to infection control concerns about wet areas and body fluids getting into the below floor space.
Specific strategies to provide capacity to accommodate varied and changing uses included:
All systems generally provide 20-25% spare capacity from source to distribution, e.g., spare electrical circuits;
Horizontal “zoning” of MEP systems pathways in the space above suspended ceiling.
Looping of piping (with shut-off valves), supply and exhaust ducts, provided redundancy and ability to isolate sections for modifications.
Plumbing location below floor slab and above suspended ceilings strived to avoid placement above sensitive areas (e.g., surgery and procedure suites) and above terminal HVAC units.
Use of chilled beams in clinical and office areas provide space planning options (and energy savings).
To date, the systems have provided consistent and reliable support to the operation of the facilities. Since opening day, Portland has experienced record high temperatures several times and the building has performed well, as reported to project design engineers.
Base Building Concepts
A wide variety of potential future changes were considered to test the base buildings’ capacity to accommodate varied and changing uses. A retrospective comparison to Open Building concepts follows, referring to the main principles of capacity analysis: Each area allows for several different layouts: The presence of many ambulatory programs in the building demonstrates provision for different layouts. Furthermore, for each program, the project team in IDE events was required to develop a number of functional layouts. For the few ambulatory programs not present, project team experience determined if good layouts were possible and even hospital program layouts were tested. Some programs if considered in the future, e.g., Magnetic Resonance Imaging, MRI, and audiology booths would require specific structural modifications as typical for such renovations. Radiation oncology would not be feasible due to extreme weight of radiation shielding.
It must be possible to change the floor area, either by additional construction (vertical or horizontal) or by changing the boundaries of the units of occupancy: Within CHH-2, there are programs that occupy full and partial floors. Program or suite boundaries and corridor locations can easily change as program space needs change. Horizontal expansion is not possible at the lower levels, due to property lines and public rights-of-ways, nor at upper levels where the building is at the maximum dimensions according to the existing zoning code. Vertical expansion is not provided for, though one floor was added during design. The ever-tightening seismic requirements of the Pacific coast have left many buildings planned for vertical expansion unable to do so without disruptive upgrade renovations, therefore building owners have generally declined to use this strategy.
Buildings should be adaptable to both residential and non-residential functions, within reason: OHSU is a client with buildings over 100 years old that are still in original use, and the university seldom demolishes buildings. Therefore, it is not anticipated that residential use would be sought. The presence of research offices demonstrates the building works well as general office use.
It should be noted that the project team did study potential conversion to other hospital uses at varying times in the design process (driven by reimbursement changes), but each time such a potential conversion was not pursued due to programmatic type issues, e.g., need for emergency department on first floor, which was not available due to other necessary ground floor functions, Fire Life Safety upgrades, increased seismic code requirements for hospitals as “essential use facilities” and impact on the project business case.
In conclusion, based on capacity to accommodate varied and changing uses of similar buildings and CHH-2’s design and planning improvements, it is fully anticipated the building will serve OHSU’s ambulatory needs for decades.
Final Design














Since Completion
Since opening four years ago, post-occupancy evaluation has occurred, with the caveat that COVID restrictions closed the facility down in early 2020 and utilization has been impacted since reopening later in that year. There has not been a need for renovations to the facility to test its ability to accommodate change. Early staff and patient feedback was positive, before COVID impacts. Patient satisfaction scores met or exceeded project goals.

Acknowledgments
Project major team members:
Owner: Oregon Health & Science University
Architect and Interiors: Zimmer Gunsul Frasca Architects, LLP
General Contractor: Hoffman Construction Company
Structural and Civil Engineers: KPFF Consulting Engineers
Mechanical and Electrical Engineers: Affiliated Engineers, Inc.
Landscape Architects: Place
Contributors: Karl Sonnenberg AIA ACHA, ZGF
Photography & Graphic Credits:
Figure 1: Courtesy of ZGF Architects LLP; © Eckert & Eckert
Figures 2-13: Courtesy of ZGF Architects LLP
Figure 14: Courtesy of ZGF Architects LLP; © Eckert & Eckert
Figures 15: Courtesy of ZGF Architects LLP; © Eckert & Eckert
Figure 16: Courtesy of ZGF Architects LLP; © Bruce Damonte